https://www.gosh.nhs.uk/conditions-and-treatments/procedures-and-treatments/treatment-for-blood-clots--thrombolysis-and-thrombectomy/
Treatment for blood clots – thrombolysis and thrombectomy
Information about how a blood clot is diagnosed and the forms of treatment – thrombolysis and thrombectomy – that may follow. It describes what to expect when your child has treatment for a blood clot at Great Ormond Street Hospital (GOSH).
What is a blood clot and why do they form?
Blood contains cells called platelets and a substance called fibrinogen – these help the blood to clot. Normally, clotting is a good thing as it prevents us loosing too much blood from an injury like a cut or a graze. However, when a blood clot forms inside the body it can disrupt blood flow and can cause serious problems.
Our blood carries oxygen. If a blood clot forms within a blood vessel, it can deprive the part of the body supplied by the blood vessel of oxygen, which can lead to tissue damage if untreated.
If a blood clot forms inside a vein and blocks it, the part of the body supplied by that vein becomes swollen as the blood is unable to flow back towards the heart.
If one forms in an artery, the blood cannot reach the area supplied by the artery.
Blood clots can form for many reasons. Some people’s blood is ‘stickier’ than others, because of other medical conditions they have, or because of a family tendency to form blood clots. Clots can also form after an operation, particularly if a person cannot move around as normal.
How is a blood clot diagnosed?
Often a blood clot is suspected while your child is still in hospital. If the doctors suspect your child has a blood clot, they will ask the doctors from IR to diagnose it using various imaging techniques. Usually, they carry out an ultrasound scan first, or occasionally MRI or CT scans.
How are blood clots treated?
Once the clot has been identified, there are three ways that it can be treated whilst under GA:
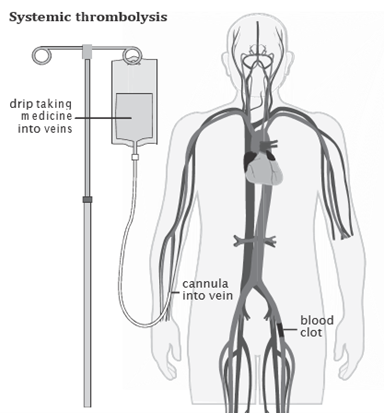
- Systemic thrombolysis – a clot-busting medicine is given through a cannula (thin plastic tube) into a vein in your child’s hand or foot. The medicine travels through the blood vessels breaking up clots elsewhere in the body.
- Catheter-directed thrombolysis – the clot-busting medicine is delivered into the centre of the clot over several hours or days. The medicine is given through a larger cannula inserted into the clot in a short procedure under general anaesthetic in the IR department.

- Mechanical thrombectomy – using tiny surgical tools, the doctor breaks down the clot into smaller pieces that can then be sucked out of the blood.

Which method is used depends on your child’s condition and any underlying problems. If the doctors decide that systemic thrombolysis is the best option, your child will receive an infusion of the intravenous drip while on the ward. This could take several days, and your child will have repeated blood tests to make sure it is working and to minimise the risk of bleeding. Your child may be moved to a different ward for this treatment so they can be carefully monitored.
For all these procedures, your child will need to be recovered on Intensive Care or a High dependency unit, due to the blood thinning medication they will be on post-procedure. It is safest to have the correct nursing staff to manage this.
What happens before the procedure?
Your child will need to be admitted to a bed on a ward in the hospital. The person bringing your child to the procedure should have “parental responsibility” for them. Parental responsibility refers to the individual who has legal rights, responsibilities, duties, power and authority to make decisions for a child. If the person bringing your child does not have parental responsibility, we may have to cancel the procedure.
The doctors from IR will explain the procedure in more detail, discuss any worries you may have and ask you to sign a consent form giving permission for your child to have the procedure. If your child has any other medical problems, please tell the doctors.
As a contrast dye is used in angiography/ venography and this is removed by the kidneys, tell the doctors if your child has any kidney problems. Angiography and venography is used to map the blood vessels so that there is a map to the clot before treatment begins.
Many of the procedures we perform involve the use of X-rays. Legally, we are obliged to ask anyone over the age of 12 whether there is any chance they might be pregnant, and we will also ask for the first date of their last period (if started). This is to protect babies in the womb from receiving unnecessary radiation.
An anaesthetist will visit to talk to you about your child’s anaesthetic.
Preparing for anaesthetic
Your child needs to be fasted for the procedure for the general anaesthetic.
As a general rule:
Food and milk:
- Breast-fed babies- can have their last feed three hours before the procedure. Breast milk is digested faster than solid food or formula.
- Bottle-fed babies and children- can have their last milk feed, food or milk drink, six hours before the procedure. They should not have any food or milk after this time.
Water:
- All babies and children can have a drink of water (but no other fluids), until one hour before the procedure.
It is equally important to keep giving your child food and drink until those times to ensure they remain well-hydrated and get adequate nutrition. This may involve waking your child in the night to give them a drink which we recommend.
Please follow these instructions carefully, otherwise your child’s procedure may be delayed or even cancelled.
What does the procedure involve?
For thrombectomy and thrombolysis procedures, once your child is under general anaesthetic, the doctor will use angiography/venography to map your child’s blood vessels and identify the blood clot.
The radiologist will insert a needle into a blood vessel, using ultrasound to guide them. Some local anaesthetic is injected into the skin first, to make the area numb for a few hours, and a very small cut is made in the skin, though which the needle is placed. A soft guide wire is threaded over the needle, which is then removed. Finally, a catheter (thin plastic tube) is threaded over the guide wire into the artery, and the guide wire is removed.
The catheter is then threaded through the arteries or veins until it is in the area needed. X-rays and contrast are used at various points to guide the catheter in the right direction and to check that it has reached the area of the blood clot. The doctors will then place a catheter into the centre of the clot while your child is still under general anaesthetic. The catheter will be connected to an infusion (drip) of clot-busting medicine, and your child will be transferred to an intensive care or high dependency unit where the infusion will continue to be given.
Mechanical thrombectomy may also be carried out during the procedure. This involves the use of a very small mechanical device mounted on a soft plastic catheter. The catheter is placed inside the blood clot in the artery or vein. The mechanical device is controlled by a machine outside the body. It travels along the blood vessel breaking down and sucking out the clot. This often allows the clot to be broken down more quickly than by just relying on the clot-busting medicine. In many cases, the doctors will use mechanical thrombectomy during the procedure and follow this up afterwards with catheter-directed thrombolysis on the ward.
What happens after the procedure
After the procedure and during the on-going clot-busting medicine infusion on the ward, your child will be closely monitored for side effects, due to the risk of bleeding. The doctors will come to check your child’s progress regularly and will give you some information about what they have done during the procedure.
Your child will need blood tests every three to four hours and repeated imaging scans in the IR department to see if the clot is dissolving as planned. These scans are usually done while your child is awake, by injecting some contrast (dye) through the infusion catheter in the blood vessel.
They will also need to wear special knee or thigh length socks which compress the legs preventing further clots forming. These can be uncomfortable, particularly when putting them on or taking them off, but they work very well.
Other medicines, sometimes given by injection, may also be needed.
Once it is clear that the clot is dissolving and the clot-busting medicine has finished, your child will be moved out of the intensive care or high dependency unit back to a normal ward, and the catheters will be removed.
Are there any risks?
Your child will be having the procedure under general anaesthetic. Every anaesthetic carries a risk, but this is extremely small.
The procedure may involve the use of X-rays. The levels that are used are low dose and therefore low risk. If you have any concerns regarding the use of radiation, please discuss this with the person performing your procedure beforehand.
The clot-busting medicine used in systemic or catheter-directed thrombolysis works by activating the proteins in your child’s blood that normally break clots down and therefore the risk of this medicine is bleeding. Any recently formed blood clot in the body will be broken down by this medicine and therefore there is a greater risk of bleeding within a few days of surgery as the body will not have healed yet.
As the drug can cause significant changes in how the blood clots, your child will need blood tests every four hours whilst they are receiving the medicine. If the medicine is given via a cannula into a vein, we tend to give the drug for around six hours and then re-assess how well it has worked before possibly repeating the infusion. If the medicine is given through a catheter directly into the centre of the clot, we are able to use a much smaller dose and therefore we can keep the medicine going for longer but still need to do frequent blood tests. While your child is receiving the clot-busting medicine, if they have any bleeding symptoms or the blood results are significantly abnormal, we will stop the medicine straight away.
Are there any alternatives?
The main alternative is to leave the clot in place and treat with anticoagulation with either heparin (injections) or warfarin (tablets) which prevent the clot from increasing and allow the body to gradually deal with the clot and open up other blood vessels around it.
However, long term blockage of a blood vessel can cause long term damage to the limb. If the blood clot formed because your child has had to have frequent central venous access devices, leaving the clot in place could reduce future access to the blood vessels.
Occasionally, the blood clot may need to be removed using open surgery, but this carries additional risk of bleeding and infection.
What do I need to look out for at home?
You should call the hospital if:
- The area looks red, swollen and feels hotter than the surrounding skin.
- Your child has weakness in the limb
- There is significant bleeding
- Your child has a temperature of 38⁰C or higher.
You can call the ward by calling the GOSH switchboard and asking for the ward your child was discharged from.
Telephone: 020 7405 9200
If you are unable to get through, please call NHS111 by dialling 111.
Contact information
If you have any questions, please speak to you child’s doctor or nurse or call Interventional Radiology:
Telephone: 020 7405 9200